Indication/Technique
Indication
The hip X-ray is used primarily to demonstrate/exclude a fracture. Hip X-rays are also frequently opted for as initial test in chronic hip symptoms, e.g. osteoarthritis.
Technique
The hip joint can be imaged under various angles. A standard hip X-ray examination generally includes an anteroposterior (PA) image and a lateral image. Ideally, the AP image shows both hip joints (which strictly speaking makes it a pelvis X-ray) to allow comparison with the other hip. The lateral direction may be opted for in axiolateral images or a frog leg lateral image. The various directions are explained in more detail below.
AP Image
The patient is placed on his/her back and the X-rays will pass through the hip joint from anterior to posterior (fig. 1). The leg is internally rotated 15˚ - 20˚ to achieve femoral anteversion. This will extend the femoral neck (collum), improving its evaluability. When the leg is rotated externally, the greater trochanter will project over the neck and improve imaging of the lesser trochanter (fig. 2).


Lateral Image
There are various techniques for lateral imaging. The most commonly used images are the axiolateral image, the frog-leg lateral image and the Lauenstein image.
Axiolateral image
The patient is placed on his/her back. The unaffected hip is abducted and lifted (using a cushion/block as support), allowing a medial view of the affected hip (fig. 3). The X-ray machine is positioned so as to direct the X-ray beams exactly through the femoral neck (horizontal beam), achieving optimal unobstructed images and minimizing overprojection of the lesser/greater trochanter.
The primary benefit is that the patient can leave the painful leg flat. After trauma or in immobile/postoperative patients therefore, the axiolateral image is first choice for lateral imaging.
The primary benefit is that the patient can leave the painful leg flat. After trauma or in immobile/postoperative patients therefore, the axiolateral image is first choice for lateral imaging.


Note: it is important not to make a frog-leg lateral image/Lauenstein image if a fracture or hip luxation is suspected. This is very painful and may complicate the fracture/luxation.
Normal anatomy
The proximal femur is formed by the proximal femoral shaft, greater/lesser trochanter, femoral neck and femoral head. The hip joint is a ball (= femoral head) and socket (acetabulum) joint. The acetabulum is formed by three fused ossal structures: the illium, ischium and pubis (complete bony fusion is achieved at the age of 20-25 years).
The artery in the round ligament (ligamentum teres) supplies the femoral head with blood, but the primary blood suppliers are the medial/lateral femoral circumflex arteries originating in the deep femoral artery (a. femoralis profunda
The artery in the round ligament (ligamentum teres) supplies the femoral head with blood, but the primary blood suppliers are the medial/lateral femoral circumflex arteries originating in the deep femoral artery (a. femoralis profunda

The round ligament is an intra-articular ligamentary structure connecting the femoral head with the acetabulum (via the femoral head fovea). The exact relevance and function of the ligament are as yet not fully understood. One of the theories is that the ligament has a stabilizing function and that a rupture may lead to instability.
The hip joint is surrounded by a firm joint capsule. The capsule surrounds the hip joint and a large part of the femoral neck (fig. 7), with several ligaments and muscles providing additional stability.
The hip joint is surrounded by a firm joint capsule. The capsule surrounds the hip joint and a large part of the femoral neck (fig. 7), with several ligaments and muscles providing additional stability.

AP Image
The trochanter is formed by the greater and lesser trochanter. Both are posterior structures; the greater trochanter is at the posterolateral side and the lesser trochanter at the posteromedial side.
When the hip is rotated internally, the projection of the greater trochanter over the femoral neck is minimized, improving visibility of the contours of the greater trochanter and femoral neck (fig. 8). The opposite happens with the lesser trochanter; visibility improves on external rotation and decreases on internal rotation.The femoral neck and greater trochanter need to be assessed reliably, which is why AP images are routinely made in 15˚ - 20˚ internal rotation (see also Technique section).
A normal femoral head has smooth contours and is covered with cartilage (note: the cartilage itself is invisible on X-ray). There is a small impression in the medial side of the femoral head: the femoral head fovea. The fovea is not covered with cartilage and includes the round ligament and the round ligament artery. When the hip is rotated internally, the projection of the greater trochanter over the femoral neck is minimized, improving visibility of the contours of the greater trochanter and femoral neck (fig. 8). The opposite happens with the lesser trochanter; visibility improves on external rotation and decreases on internal rotation.The femoral neck and greater trochanter need to be assessed reliably, which is why AP images are routinely made in 15˚ - 20˚ internal rotation (see also Technique section).
In a normal hip joint, the acetabular roof covers the entire femoral head (good coverage). The anterior and posterior wall of the acetabulum project over the femoral head and may not be easily discernible on a PA image (f

Some helpful lines can be identified in the AP image to distinguish normal anatomy from pathology (fig. 10):
- iliopectineal line/iliopubic line: line at the inside of the ilium, continuing at the bottom along the cranial rim of the superior pubic ramus.
- ilioischial line: runs along the inner rim of the ilium, at the bottom (via the tear drop configuration) continuing along the medial side of the ischium.
- Shenton line: an imaginary line at the bottom of the superior pubic ramus, continuing along the inferomedial side of the femoral neck.
- tear drop: located at the medial side of the femoral head and also known as the U-figure. The lateral line is formed by the cortical rim of the acetabulum and the medial line through the cortical medial rim of the acetabulum (= quadrilateral plate, where it meets the lesser pelvis), see also figure 11.
- anterior/posterior wall of the acetabulum: these lines are formed by the lateral rims of the anterior and posterior acetabulum respectively. They project over the femoral head and can be difficult to identify.
The above lines should be smooth and uninterrupted. If a line is absent or abnormal, local pathology should be suspected, e.g. a fracture or ossal lesion.

Trabecular pattern
In the femoral neck, the trabecular pattern can also be observed. The trabeculae in the bone provide support during stress and develop in a pattern related to the degree of stress; trabeculation increases in areas with more stress.
There is a radiolucent area at the bottom of the femoral neck (located between the three trabecular groups). This anatomical area contains relatively limited trabeculation and is termed Ward’s triangle – not to be confused with an osteolytic lesion (fig. 12).
The greater trochanter and the craniolateral & inferomedial part of the femoral head are somewhat more lucent also because of relatively limited trabeculation; this is physiological.
In a normal hip, the bone trabeculae are uninterrupted and smooth. If they are interrupted, a fracture should be suspected (see Pathology section).
There is a radiolucent area at the bottom of the femoral neck (located between the three trabecular groups). This anatomical area contains relatively limited trabeculation and is termed Ward’s triangle – not to be confused with an osteolytic lesion (fig. 12).
The greater trochanter and the craniolateral & inferomedial part of the femoral head are somewhat more lucent also because of relatively limited trabeculation; this is physiological.
In a normal hip, the bone trabeculae are uninterrupted and smooth. If they are interrupted, a fracture should be suspected (see Pathology section).

Lateral Image
In axiolateral imaging, attempts will be made to optimally image the femoral neck (fig. 13).


Checklist
The following points may be used as a guide to assess a hip X-ray.
General:
- Technique: has everything been imaged correctly; is it suitable for evaluation? Can the question be answered?
- Bone mineral density? Ossal lesions?
- Check the cortex; cortex interrupted? cortex destruction?
- Normal trabecular pattern on femoral head/neck?
- Abnormal iliopectineal line, ilioischial line, tear drop or Shenton line?
- Hip joint: position? osteoarthritis? Asymmetry when compared to the other hip?
- Abnormalities outside the hip joint?
- Changes versus previous examinations?
Pathology
Proximal Femoral Fractures
Avascular Necrosis
Acetabular Fracture
Hip Luxation
Osteoarthritis
Hip Prosthesis
Proximal Femoral Fractures
Proximal femoral fractures occur fairly regularly in elderly osteoporotic patients and may be caused by a simple fall. In younger people, they are more commonly caused by high-energy trauma.
The classical clinical presentation of a proximal femoral fracture is shortening and exorotation of the affected leg.Characteristics of a proximal femoral fracture:- the lesser trochanter is more easily identified by the exorotation of the leg
- cortex interruption and/or fracture gap
- a vague dense (‘white’) line in an impacted fracture
- disrupted bone trabeculation in the femoral head/neck
- disrupted Shenton line
Proximal femoral fractures may be subdivided as follows (fig. 15):- femoral neck fracture (= intracapsular fracture)
- pertrochanteric/intertrochanteric fracture
- isolated fracture of the greater and lesser trochanter
- subtrochanteric fracture

Intracapsular Fractures
The femoral neck is the weakest point of the proximal femur; it is an intracapsular fracture and may be further subdivided into the subcapital, midcervical and basicervical types (fig. 15).
Intracapsular fractures are associated with a high risk of intracapsular vascular damage. This may cause devascularization of the femoral head and eventually avascular necrosis. As a result of both the interrupted blood supply and limited intrinsic stability, intracapsular fractures also entail a higher risk of nonunion/malunion as compared to extracapsular fractures.The Garden classification is commonly used to categorize femoral neck fractures (fig. 16):- Garden I: incomplete fracture associated with some valgus of the femoral head. The valgus position interrupts/disrupts the trabecular pattern in the head/neck (fig. 17). Also valgus impacted fractures come under type I.
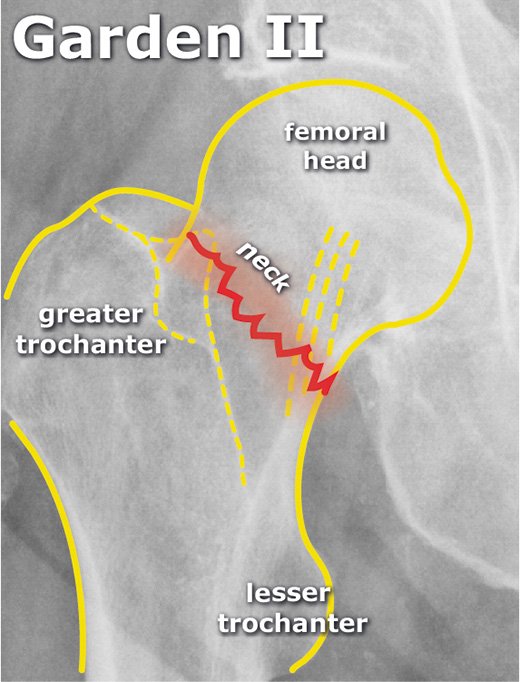
- Garden II: complete subcapital fracture without dislocation. Because of the anatomic position of the head, there is no disruption of the trabecular pattern in the head/neck (fig. 18).
- Garden III: complete subcapital fracture with some dislocation. The head has some varus angulation.
- Garden IV: complete subcapital fracture with full dislocation (fig. 19).


Extracapsular Fractures
Pertrochanteric femoral fractures occur between the greater and lesser trochanter. These fractures are frequently associated with significant dislocation (also because of muscular traction) and will therefore almost always require surgery (fig. 20).
The risk of avascular necrosis of the femoral head is smaller as compared to intracapsular fractures.
When there are no separate fractures of the lesser and greater trochanter, we use the term intertrochanteric femoral fracture.
An isolated fracture of the greater trochanter may be caused by direct trauma.
An isolated fracture of the lesser trochanter is rare and may occur as an avulsion fracture of the iliopsoas muscle at a young age. Important: in adults with an isolated lesser trochanteric fracture, always beware of a pathological fracture (such as a bone metastasis).
Subtrochanteric Fracture
This fracture type is usually caused by high-energy trauma in young patients. The fracture is located caudally to the trochanters.
There may also be a combined intertrochanteric/subtrochanteric femoral fracture (fracture involves both the lesser/greater trochanter and the subtrochanteric region), see figure 21. The strong mechanical forces of the body frequently destabilize the fracture and internal fixation will be opted for.

- Note:
Proximal femur fractures can be very subtle, especially in the case of impacted femoral neck fractures (fig. 22). Osteophytes (“collar osteophytes”) in coxarthrosis can be easily mistaken for a femoral neck fracture (and vice versa).
When in doubt on the hip X-ray with a strong clinical suspicion, a CT scan can be made for additional analysis.  Fracture type, degree of dislocation and patient age are important factors determining treatment.
Fracture type, degree of dislocation and patient age are important factors determining treatment.
Femoral neck fractures impacted in valgus (Garden I) are relatively stable and are frequently treated conservatively (also guided by the surgeon’s experience/preference). In a conservative strategy, the risk of secondary dislocation should always be taken into account.
In surgical treatment, a choice can be made between fixation using osteosynthesis (a plate-screw combination or isolated screws) or prosthetic replacement of the hip joint (head-neck prosthesis, total hip prosthesis).Avascular Necrosis
A notorious complication of femoral neck fractures is avascular necrosis (AVN) of the femoral head. Traumatic damage to the supplying arteries will cause osteonecrosis.
The non-traumatic form of AVN may have many causes, including hematologic disorders (such as thalassemia and sickle cell disease), chronic corticosteroid use and chronic renal failure.
Radiologic characteristics of AVN of the femoral head (fig. 23/24):- stage I: normal/mild osteopenia as a sign of bone resorption
- stage II: mixed picture of osteopenia/sclerosis and/or subchondral cysts
- stage III: crescent sign (linear subchondral lucency) and/or cortical collapse
- stage IV: secondary osteoarthritis of the hip joint
Note: X-ray images may seem normal in the initial phase. At this point, abnormalities may be visible on MRI (this procedure will not be discussed in this course).

Acetabular Fracture
Acetabular fractures are usually caused by high-energetic trauma.
The exact classification of acetabular fractures is complex (CT scan required!) and will not be discussed further here. Roughly, a distinction is made between fractures of the posterior and anterior acetabulum. Dislocation or irregularity of the joint surface will eventually lead to early osteoarthritis (the risk of osteoarthritis depends highly on the type of acetabular fracture).
Characteristics of an acetabular fracture on a pelvis/hip X-ray (fig. 25/26):- disruption of the iliopectineal line/iliopubic line
- disruption of the ilioischial line
- disruption or asymmetry (versus contralateral side) of tear drop configuration
- disruption of anterior/posterior wall lines

Hip Luxation
Hip luxations are rare and are usually caused by high-energy trauma. A common mechanism is the so-called “dashboard fracture”; a car driver hits a flexed knee against the dashboard. In addition to a posterior hip luxation, there is frequently a fracture of the posterior acetabulum also.
In almost all (90%) cases there is posterior hip luxation.
Radiologic characteristics of posterior hip luxation (fig. 27):- femoral head is posterior and superior to the acetabulum
- greater trochanter is often projected free (as a result of internal femoral rotation)
- femoral head is somewhat smaller versus the contralateral side because it is closer to the plate (lower amplification factor with diverging X-rays)
The luxated hip should be repositioned as soon as possible; prolonged hip luxation increases the risk of eventual avascular necrosis of the femoral head.
Coxarthrosis
Osteoarthritis is a complex disease characterized by synovitis, cartilage wear, reactive bone formation (osteophytes) and subchondral abnormalities. It is associated with a diversity of symptoms. Patients may complain about progressive load-dependent pain and/or reduced hip function. Osteoarthritis of the hip is termed coxarthrosis.
The osteoarthritis may be primary with no obvious identifiable cause. Secondary osteoarthritis develops after e.g. a fracture.
Radiological characteristics of osteoarthritis (fig. 28):- Narrowing of the joint space secondary to cartilage loss
- Subchondral sclerosis (increased bone production secondary to increased pressure with cartilage loss)
- Osteophyte formation (bone exostoses attempting to increase the joint surface)
- Subchondral cysts (secondary to microfractures of the subchondral bone and pressure of the synovial fluid).

Hip arthroplasty
A hip prosthesis is a treatment option for disabling osteoarthritis. In most cases, both the acetabulum and the femur are replaced – the total hip arthroplasty (THA). Both cemented THA and uncemented THA may be opted for.
If the fracture is in the femoral neck, and if the patient is older (and life expectancy is limited), a head-neck replacement may suffice – the hemiarthroplasty (HAP). In HAP, only the femoral head is removed and the acetabulum is preserved. See figure 29 Luxation of Hip arthroplastyA potential complication of the hip arthroplasty is luxation (fig. 30). As in a normal hip, most hip prostheses will luxate towards posterior (see also “Hip Luxation” section). This may occur as one gets up from a low chair, makes rotating movements or puts on shoes.
Luxation of Hip arthroplastyA potential complication of the hip arthroplasty is luxation (fig. 30). As in a normal hip, most hip prostheses will luxate towards posterior (see also “Hip Luxation” section). This may occur as one gets up from a low chair, makes rotating movements or puts on shoes.
With mild muscular relaxation, the hip can usually be repositioned. If not, repositioning under anesthesia may be opted for.
If hip luxations recur, repeat surgery may be considered to revise the hip arthroplasty.
- Loosening/Infection of the Hip arthroplastyDespite all precautions, a prosthesis may become infected. Patients’ symptoms may be vague and difficult to interpret.
The infection may manifest as loosening of the prosthesis.
Characteristics of prosthetic loosening on the hip X-ray:- lucent zone of > 2 mm surrounding the prosthetic material
- prosthesis migration
Characteristics of hip prosthesis infection on the hip X-ray (fig. 31):- vague periprosthetic bone resorption
- irregular bone destruction and periosteal reaction

- te: low-grade infections may have normal X-rays or simulate detachment.
All the above characteristics may be very subtle, therefore thorough evaluation of previous tests is essential.
In the case of a severe infection, the prosthesis should be removed and the hip is left without a head and neck; the so-called girdlestone situation.Periprosthetic Fracture
A fracture may occur in any type of prosthesis. Usually these are traumatic fractures (fig. 32). A fracture may also develop during surgery (e.g. in weak osteoporotic bone), however this is much rarer.
Depending on the fracture type, surgical intervention may or may not be opted for















No comments:
Post a Comment