MRI of the prostate is primarily used to evaluate prostate cancer. Your doctor will use this exam to:
Monday, 22 July 2019
What is Pulmonary Embolism?
A pulmonary embolism occurs when a blood clot moves through the bloodstream and becomes lodged in a blood vessel in the lungs. This can make it hard for blood to pass through the lungs to get oxygen. Diagnosing a pulmonary embolism can be difficult because half of patients with a clot in the lungs have no symptoms. Others may experience shortness of breath, chest pain, dizziness, and possibly swelling in the legs. If you have a pulmonary embolism, you need medical treatment right away to prevent a blood clot from blocking blood flow to the lungs and heart.
Your doctor can confirm the presence of a pulmonary embolism with CT angiography, or a ventilation perfusion (V/Q) lung scan. Treatment typically includes medications to thin the blood or placement of a filter to prevent the movement of additional blood clots to the lungs. Rarely, drugs are used to dissolve the clot or a catheter-based procedure is done to remove or treat the clot directly.
Sunday, 21 July 2019
What os Computed Tomography (CT) - Body?
Computed tomography (CT) of the body uses sophisticated x-ray technology to help detect a variety of diseases and conditions. CT scanning is fast, painless, noninvasive and accurate. In emergency cases, it can reveal internal injuries and bleeding quickly enough to help save lives.
Friday, 12 July 2019
Introduction MRI
Magnetic Resonance Imaging (MRI) is a spectroscopic imaging techniques used in medical setting to produce imaging of the inside body.
Tuesday, 9 July 2019
What patients are considered high risk patients for IV contrast for CIN?
This answer is very broad but here are some typical responses :
- The patient with a history of renal disease especially if the patient is a diabetic
- A patient on certain known nephrotoxic drugs such as aminoglycosides and amphotericin B
- Dehydrated patients regardless of the cause
- Patients with poor cardiac status including congestive heart failure
- Patients with multiple myeloma
- Patients with recent contrast injection of more than 100-120 ml in the preceding 24 hours (potential increased risk)
Do we have set cutoffs for creatinine levels and if so what are they?
Although this will vary on the patient and the importance of the study general guidelines are that for creatinines under 1.7 we will use Omnipaque-350. For creatinines of 1.8-2.1 or so when the study is needed we use Visipaque-320. Please note that we will make certain to minimize the contrast volumes in patients with the use of saline flush or just smaller volumes of contrast. On select studies we can use as little as 60 ml of contrast. Remember that there is no threshold of contrast volume for inducing CIN but it is uncommon with volumes of 100 ml or less.
Can we pretreat patients who have borderline renal function? If yes then how?
Two common regimens are the use of bicarbonate in solution as part of a prestudy ( and often post study protocol) hydration protocol
Use of N-Acetylcysteine (meta-analysis showed no advantage although recent article was more positive about its use)
Should patients be NPO for CT scanning? If yes for how long?
We like the patient to be NPO for food for a minimum of 3 hours. However, fluids are encouraged (water is best) to keep the patient well hydrated. Dehydration is a leading factor for development of CIN.
Monday, 8 July 2019
What are the common volumes of contrast used for IV injection?
With the newest 64 MDCT scanners most patients have contrast volumes in the 100-120 ml range. We find that for many applications 100 ml of contrast works fine. Please note that in the past many sites used 150-200 ml of contrast for abdominal/liver CT and CT angiography.
What are the common volumes of contrast used for IV injection?
The best site for IV access is the right antecubital fossa. This site provides a combination of optimal safety plus a good point to time delivery of contrast in studies such as cardiac CTA and pulmonary embolism studies. The left antecubital fossa would be our second choice.
We prefer an 18g angiocatheter in the antecubital fossa when possible. This typically can easily accept injection rates of 5 cc/sec without any problem. We will use a 20g when an 18g is not possible. For 20g we can inject up to 4 cc/sec safely.
What kind of IV access is ideal for use for IV contrast injection?
The best site for IV access is the right antecubital fossa. This site provides a combination of optimal safety plus a good point to time delivery of contrast in studies such as cardiac CTA and pulmonary embolism studies. The left antecubital fossa would be our second choice.
We prefer an 18g angiocatheter in the antecubital fossa when possible. This typically can easily accept injection rates of 5 cc/sec without any problem. We will use a 20g when an 18g is not possible. For 20g we can inject up to 4 cc/sec safely.
Has there been any new developments in technology that may help us high injection rates in patients who can not tolerate an 18g needle (or at times even a 20g)?
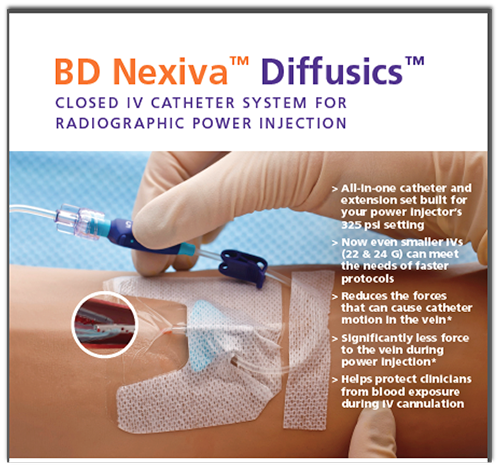
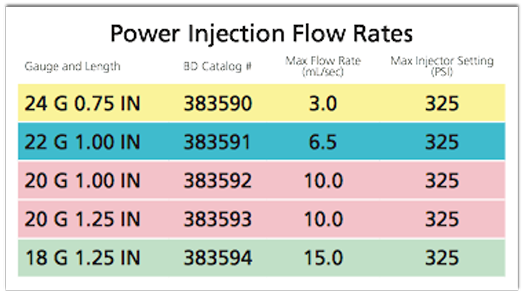
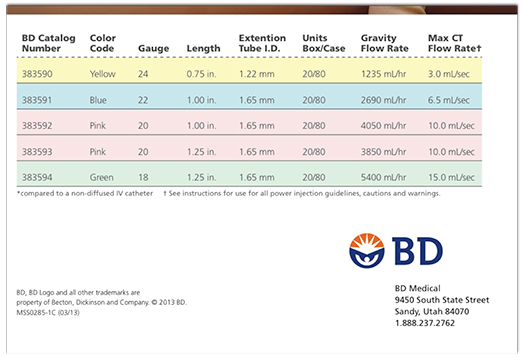
The answer is yes. This past year the Nexiva Diffusics catheter got FDA approval for use. This allow us to use smaller needles and still get high injection rates. The 20g Diffusics can inject up to 10 cc/sec and the 22g up to 6.5 cc/sec. This is a major step forward.




IV Catheter Safety
- Most IV catheters are pressure rated and usually the safety on the injector is for a pressure of 300 psi or less. Exceeding this can result in product leakage and or damage to the catheter and potentially injury to the patient
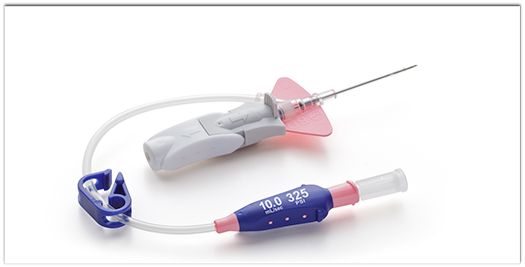
- Some of the newer generation IV catheters like the BD Nexiva Diffusics can be used to a psi of 325
- Please be certain that you are aware of what catheter you use and in practice it is ideal to use one brand only to prevent errors in setting the psi values in routine practice
"The purpose of this study was to compare the performance of a 20-gauge fenestrated catheter with an 18-gauge nonfenestrated catheter for i.v. contrast infusion during MDCT."
I.v. contrast administration with dual source 128-MDCT: a randomized controlled study comparing 18-gauge nonfenestrated and 20-gauge fenestrated catheters for catheter placement success, infusion rate, image quality, and complications.
Johnson PT, Christensen GM, Fishman EK.
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70.
Johnson PT, Christensen GM, Fishman EK.
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70.
"A 20-gauge fenestrated catheter performs similarly to an 18-gauge nonfenestrated catheter with respect to i.v. contrast infusion rates and aortic enhancement levels and can be placed in most subjects whose veins are deemed insufficient for an 18-gauge catheter."
I.v. contrast administration with dual source 128-MDCT: a randomized controlled study comparing 18-gauge nonfenestrated and 20-gauge fenestrated catheters for catheter placement success, infusion rate, image quality, and complications.
Johnson PT, Christensen GM, Fishman EK.
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70.
Johnson PT, Christensen GM, Fishman EK.
AJR Am J Roentgenol. 2014 Jun;202(6):1166-70.
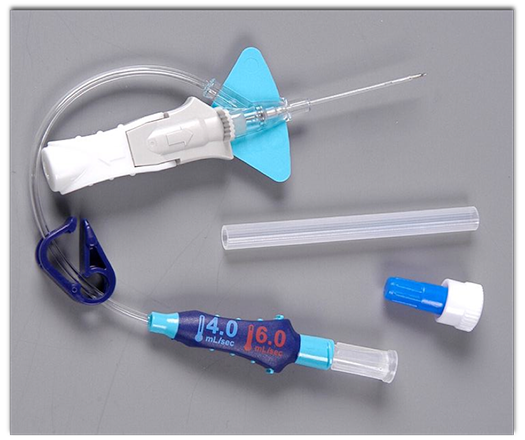
Hardware: IV Access Device
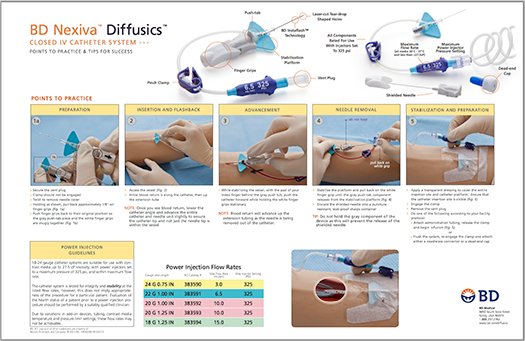
BD Nexiva Diffusics
Injection Rates
Injection Rates
BD Nexiva Diffusics
"Experienced IV starters usually achieve IV access in one attempt by tailoring IV catheter gauge to vein quality; however, target infusion rates are not likely to be achieved with 22- and 24-gauge catheters, used in nearly 1/3 of the patients in this study."
Catheter insertion for intravenous (IV) contrast infusion in multidetector-row computed tomography (MDCT): defining how catheter caliber selection affects procedure of catheter insertion, IV contrast infusion rate, complication rate, and MDCT image quality.
Johnson PT, Christensen G, Lai H, Eng J, Fishman EK.
J Comput Assist Tomogr. 2014 Mar-Apr;38(2):281-4
Johnson PT, Christensen G, Lai H, Eng J, Fishman EK.
J Comput Assist Tomogr. 2014 Mar-Apr;38(2):281-4
20 G Nexiva Diffusics
10.0 cc/sec injection rate
10.0 cc/sec injection rate
22 G Nexiva Diffusics
6.5 cc/sec injection rate
6.5 cc/sec injection rate
24 G Nexiva Diffusics
3.0 cc/sec injection rate
3.0 cc/sec injection rate
Nexiva in Use
Standard 18g vs Nexiva 20g
Nexiva Kit
20. Can any IV the patient has in place be used to inject the contrast material?
| A 18-20 g IV line can be used with the caveat that the line functions well on test injections and the line can be monitored during the injection of the contrast.
A line covered by excess tape or gauze should not be used unless the gauze or tape can be removed to access/monitor the patients injection site. Not following this rule religiously will result in errors
|
Can we use a central line or a PICC line for injection?
Hospital policies will vary but at Hopkins we have several well defined policies. They include:
- Standard PICC lines can not be used for IV injections
- Central lines can be injected by hand but not with power injectors. This policy is not a universal one
- For information purposes some sites allow power injection into central lines with a limited flow rate (2 cc/sec) or at a lower preset pressure rating on the injector
- Under no circumstances should PICCs be used with power injectors. They can shear or break.
What are some of the common normal “side effects” of IV contrast agents?
RadiologyInfo.org which is sponsored by RSNA and the ACR notes that “When an iodine-based contrast material is injected into your bloodstream, you may have a warm, flushed sensation and a metallic taste in your mouth that lasts for a few minutes.”
They then divides reactions into mild, moderate and severe. The mild reactions might be considered normal in many ways although any hives would raise concern for the next time IV contrast is used. Here is the info from RadiologyInfo .org
|
Is it ok for patients to have both an MR and a CT with contrast on the same day
This question was addressed on the RSNA site and there is no issue doing both MRI and CT the same day with Gadolinium and Iodinated Contrast.
Here is more detailed information courtesy of Richard A. Vitti MD from Medical Affairs at GE Healthcare.
CT contrast, or X-ray contrast for IV use, is usually an iodinated compound, whereas most MRI contrast media contains a heavy metal ion usually gadolinium. Iodine provides contrast by virtue of absorption of X-rays at the K-edge. Gd provides contrast in MR by changing the magnetic moment. Generally these agents distribute themselves from the vascular space to the interstitial space of soft tissues, and are elminated by glomerular filtration by the kidneys.


Are there any contrast volume limitations for the use of IV contrast?
Traditionally contrast dose for adult body CT is given in ranges of 50ml – 200ml, depending on procedure (hepatic, renal…) and iodine concentration (270mgI/ml to 400 mgI/ml). With increasing awareness of CIN and radiation dose, the trend has started to shift toward contrast dose by body weight. Some device manufacturers like Medrad (P3T) have introduced power injectors that follow a dose by weight protocol. There are a few studies published on weight-based dose for adults. Below are several examples.
Sunday, 7 July 2019
What the meaning of GFR ?
Glomerular Filtration Rate (GFR) and Creatinine Clearance (CrCl) in Health and Disease: Using Popular Formulae (September 2009)
Subscribe to:
Comments (Atom)